Friction Is the Real Talent Shortage
There is a friction surplus.
When clinicians say, “The process was exhausting,”
they’re not describing the market.
They’re describing your system.
And in distributed healthcare networks, friction compounds faster than scarcity ever could.
The Hidden Tax on Clinicians
Look at the typical hiring journey:
- Re-enter the same credentials three times
- Wait weeks for email replies
- Interview with multiple stakeholders who haven’t aligned
- Negotiate housing and logistics separately
- Complete onboarding modules that duplicate previous ones
From the employer’s perspective, this is “thorough.”
From the clinician’s perspective, it’s noise.
High performers don’t avoid rural systems, large networks, or complex organizations.
They avoid unnecessary friction.
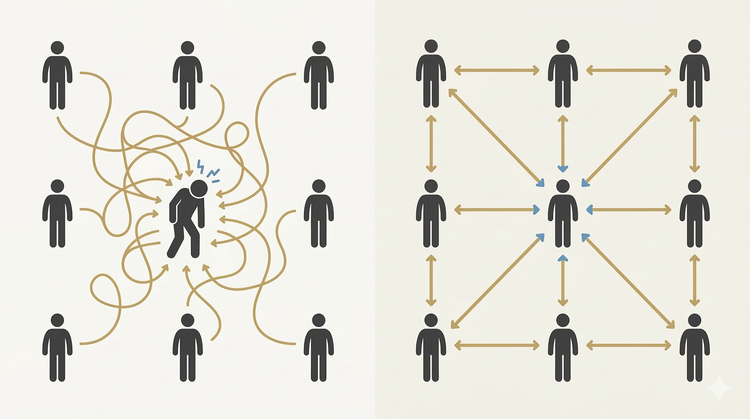
The Network Problem
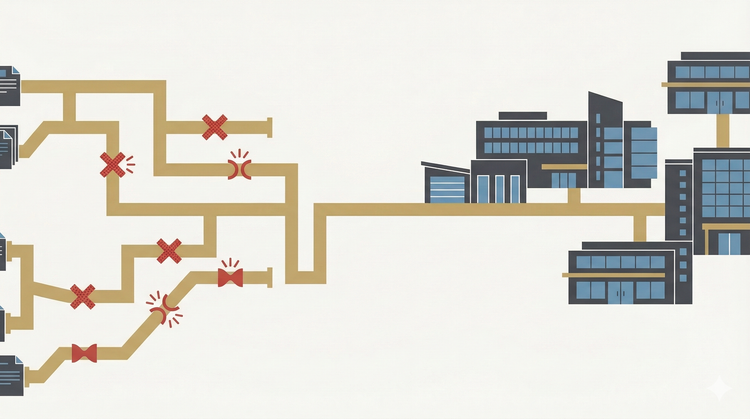
In distributed environments (hospitals, dental groups, retail health, regional systems) friction multiplies because infrastructure is fragmented.
Every site:
- Has its own paperwork
- Has its own onboarding sequence
- Has its own scheduling logic
- Protects its own leads
This feels autonomous.
It’s actually expensive.
Because every time a clinician drops out of your process, the cost isn’t just the lost hire.
It’s the reputation damage.
Friction spreads through word-of-mouth faster than marketing ever can.
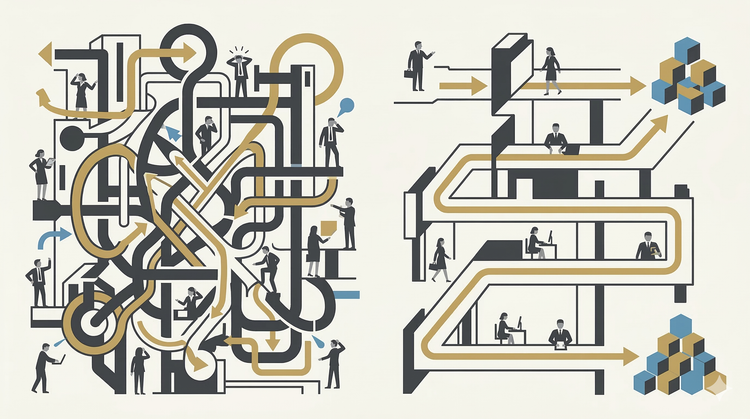
The Architecture Shift
When we redesigned recruitment systems in high-constraint environments, we stopped asking:
“How do we recruit more?”
And started asking:
“Where is the process heavy?”
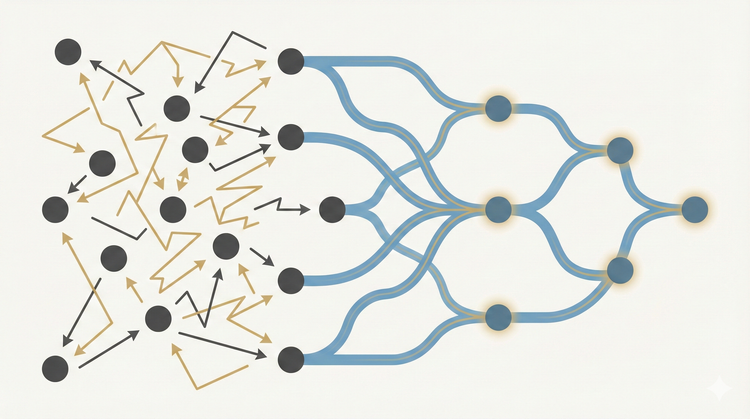
Instead of optimizing effort, we optimized flow.
Three structural shifts changed everything:
1. Credential Once, Work Anywhere
We centralized credentialing across sites.
One submission.
One verification.
Network-wide eligibility.
The impact wasn’t administrative efficiency.
It was psychological relief.
Clinicians stopped feeling like temporary contractors.
They felt portable.
2. Internal Handoff, Not Restart
If a clinician wasn’t a fit for one location, we didn’t restart the process.
We rerouted them.
No new forms.
No repeated interviews.
No reputational reset.
A “no” became a redirect.
The system kept momentum.
3. Standardized Onboarding Rituals
Every site had autonomy.
But the onboarding architecture was unified.
Clear expectations.
Predictable communication cadence.
Defined first-week structure.
When clinicians know what the first 30 days will feel like, anxiety drops — and acceptance rates rise.
The Compounding Effect
When friction drops:
- Time-to-decision shortens
- Offer acceptance increases
- Return rates improve
- Internal referrals grow
The system becomes easier to work in.
That reputation becomes your moat.
You don’t need louder marketing.
You need smoother infrastructure.
The Executive Lens
Most leaders focus on talent acquisition metrics.
Few audit talent experience architecture.
If you run a distributed network, ask:
- How many times does a clinician repeat information?
- How many people own the same step?
- Where does momentum die?
- If a candidate says “no” at Site A, do they leave your ecosystem?
The margin is rarely in sourcing.
It’s in simplification.
Remove friction, and capacity increases without adding headcount.
That’s not recruitment.
That’s system design.
EXECUTIVE SUMMARY
The Problem
Distributed networks lose clinicians not because of scarcity, but because of process friction.
The Shift
Replace site-level autonomy in onboarding and credentialing with coordinated infrastructure.
The Outcome
Lower drop-off, higher acceptance, stronger retention, and reputational compounding.